
As yoga teachers, it is our job to assist people in moving their body in mindful ways that will bring overall physical and mental well-being. A big part of this responsibility entails preventing injury whenever possible. To this aim, yoga teachers use a myriad of alignment cues designed to protect the body from injury. Some of these cues are good advice. Others seem to make little sense. For example, why should one flex the ankle to protect the knee in a hip opening pose? In order to understand whether this is a useful alignment cue, we must explore the effect that hip opening poses have on the knee, and how movement at the ankle may or may not mediate this effect.
Anatomy of the knee
Image 1 shows the bones and joints of the knee. The thigh bone is the femur. There are two bones in the lower leg - the larger, weight-bearing tibia, and the smaller, non-weight bearing fibula. The patella, or knee cap, is a bone that is embedded in the tendon of the quadruceps muscle. It is in the front of the knee joint. These bones join together in various places. The main knee joint is where the femur and tibia meet (tibiofemoral joint) and the secondary knee joint is where the femur and patella meet (patellofemoral joint). There is a third joint in the area between the two lower leg bones (tibia and fibula). This joint is called the proximal tibiofibular joint (PTFJ). The anterior and posterior fibular ligaments bind the fibula to the tibia (Image 2). [Side note: The tibia and the fibula join again near the ankle at the distal tibiofibular joint (DTFJ)].
There are a number of muscles, ligaments, nerves and blood vessels that cross the knee joint. One that is important for knee stability is the lateral collateral ligament (shown in image 1) that passes from the femur to the fibula on the outside of the knee.

Image 1: View of the right knee from the front/side showing the femur, tibia, fibula and patella.
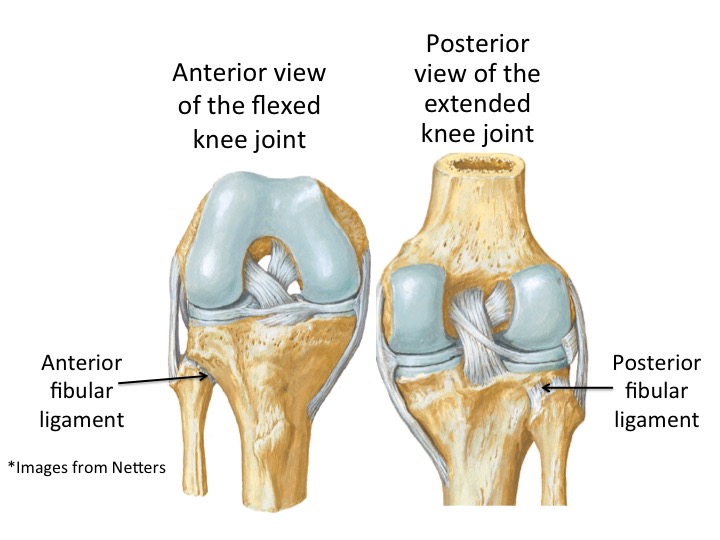
Image 2: Anterior and posterior views of the knee showing the fibular ligaments.
What happens to the knee in a hip opener with lateral rotation?
If all you are doing is laterally rotating at the hip, then there is no risk to the knee. For example, if you were to lie on your back with your right leg lifted into the air and rotate your thigh outwards, you would be stretching your hip rotator muscles. It probably wouldn’t be a very big stretch because you don’t have much leverage to rotate, but the knee would be safe because the only action is happening at the hip. But if you wanted to deepen your stretch by bending your knee and drawing your foot in close to your body (referred to here as “figure-4 position”), then you introduce movement at the knee joint, even though the target area is the hip. A figure-4 position can include the reclining position described, the standing pose of knee over ankle with both knees bent, the hip opening stretch known as pigeon prep (eka pada raja kapotasana), firelog pose or agnistambhasana (Image 3) among others. In all of these positions, you are using the foot and lower leg (tibia and fibula) as leverage to create a greater external rotation at the hip.
When you pull your foot in towards your body for the figure-4 position, you put tension on the outer knee joint and compression on the inner knee, a position known as a varus alignment. When varus alignment is chronic and affects a person’s stance and/or mobility, it is known as varus deformity. Varus deformity is often congenital, but can also arise in adults due to disease. Most of the research on this condition addresses the fact that this is a chronic condition and has its own set of problems that arise because of it. For example, varus alignment that persists over time can lead to osteoarthritis on the medial (inside) surface of the knee joint because of the increased pressure there.
In a healthy knee, varus alignment is prevented by several structures, including the lateral collateral ligament (Image 1). However, once the knee bends, this ligament becomes lax, which allows for a greater degree of opening in the lateral knee. However, neither the increased varus alignment or the general laxity at the outer knee would be immediately problematic for a student, unless the student pushes too hard and experiences pain in the joint. Joint pain is nearly always a clear sign that you should come out of a pose.

Image 3: Fire log pose (agnistambhasana) showing the figure-4 position of the left leg. Image courtesy of Courtney Long Photography.
Anatomy of the ankle

Image 4: x-ray of the right ankle.
The ankle is a complex region that involves the interaction of several bones to create movement. For our purposes, we are going to focus on the true ankle joint, which is between the two bones of the leg (the tibia and the fibula), and the talus, which is a bone of the foot. The x-ray (Image 4) shows the ankle joint of a right leg. The distal tibia and fibula are bound together via ligaments at the distal tibiofibular joint (DTFJ) and move as a unit over the talus to produce movement in a single plane.

Image 5: Superior view of the talus demonstrating its irregular shape
However, the talus is irregularly shaped (Image 5). So as the tibia and fibula move along its length, they can change their relationship to one another. This change in relationship is reflected in both the distal (ankle) and proximal (knee) regions.
What effect does flexing the ankle have on the knee joint?
Flexing the ankle does not have an effect on the knee joint (either the patellofemoral joint or the tibiofemoral joint). However, flexing the ankle does affect the position of the proximal tibiofibular joint (PTFJ).
When the knee flexes, as it does in the figure-4 position, the proximal fibula glides forward relative to the tibia due in part to the release of the lateral collateral ligament (Ogden, 1974a, Andersen, 1985). However, when the ankle is flexed, the PTFJ rotates externally (Ogden, 1974b, Eichenblat and Nathan, 1983, Bozkurt et al., 2003, Andersen, 1985) and fibula lifts slightly (Moore et al., 2010). This can have the effect of minimizing strain on ligaments that attach to the fibula, including the anterior and posterior fibular ligaments (see Image 2).
Strain or tension in the anterior and posterior fibular ligaments could result in tearing and/or dislocation. If they become loose, or tear, then the proximal fibula can pull away from the tibia. However, dislocation of the proximal fibula is very rare and typically happens only in high-impact events such as falls. The possibility still remains that these ligaments can stretch in this position and compromise the integrity of the joint.
Does flexing the ankle actually protect the knee?
Probably not. At most, it stabilizes the PTFJ. But that joint is not much in danger of dislocation in a static figure-4 position.
But flexing your ankle does require in most cases that the ankle joint be better situated on top of the knee, which will increase the intensity of the stretch of the muscles of the hip. So this instruction can still be useful to yoga students because it allows you to experience a depth in the pose that you might not otherwise.
And flexing the ankle can definitely help protect and stabilize the ankle if a student is pulling too hard on the foot in order to get it up onto the knee.
Articles referenced
Andersen K. 1985. Dislocation of the superior tibiofibular joint. Injury. 16:494-498.
Bozkurt M, Yilmaz E, Atihan D, Tekdemir I, Havitcioglu H, Gunal I. 2003. The proximal tibiofibular joint: An anatomic study. Clinical orthopedics and Related Research. 406:1:136-40
Claes S, Vereecke E, Maes M, Victor J, Verdonk P and Bellemans J. 2013. Anatomy of the anterolateral ligament of the knee. Journal of Anatomy. 223:321-328.
Eichenblat, M and Nathan, H. 1983. The proximal tibiofibular joint. An anatomical study with clinical and pathological considerations. Int orthop. 7:31-39
Moore KL, Dalley AF, Agur AM and Limb L. 2010. Clinically Oriented Anatomy.
Ogden, JA. 1974a. Subluxation and dislocation of the proximal tibiofibular joint. Journal Bone Joint Surg Am. 56: 145-154
Ogden, JA. 1974b. The anatomy and function of the proximal tibiofibular joint. Clinical orthopedic Relat Res. 101:186-191
Sarma, Amitav, Borgohain, Bhaskar and Bishwajeet Saikia. 2015. Proximal tibiofibular joint: Rendezvous with a forgotten articulation. Indian Journal of Orthopaedics 49.5 (September - October, 2015): p489